The knees are strong and complex. When we run or jump, our knees help support our weight. It lets us bend, flex, and rotate our legs. However, it is vulnerable to injury if we land the wrong way, change direction fast, or get hit hard. The knees consist of the anterior (front) and posterior (back) ligaments. When one or any of them gets torn, it can cause pain and temporary disability.
This post is going to cover the difference between the two. It will also discuss the anatomy, cause, symptoms, treatment, and rehabilitation. By the end of this blog, you should have better understanding of what to do and how to recover as quickly as possible.
Anatomy
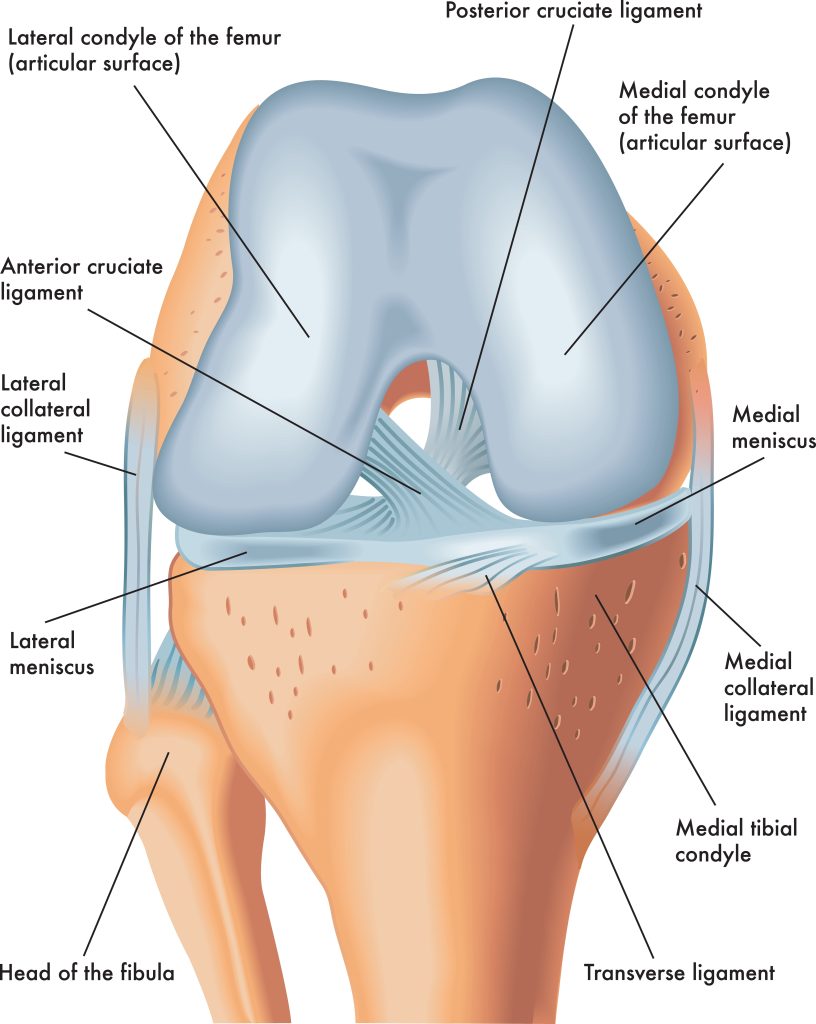
There are two cruciate ligaments that hold your knees together, the ACL and PCL. These ligaments cross one another, making an “X” at the center of the knee. With this shape, the knee can flex and extend, but with limited side-to-side movement. The PCL is found on the front side of the knee, while the ACL is at the back. They connect the tibia to the femur.
The ACL prevents the tibia from sliding further forward along the femur. In contrast, the PCL prevents the tibia and femur from sliding backward.
Causes
It is possible to sustain a torn ACL or PCL in a sports accident.
ACL
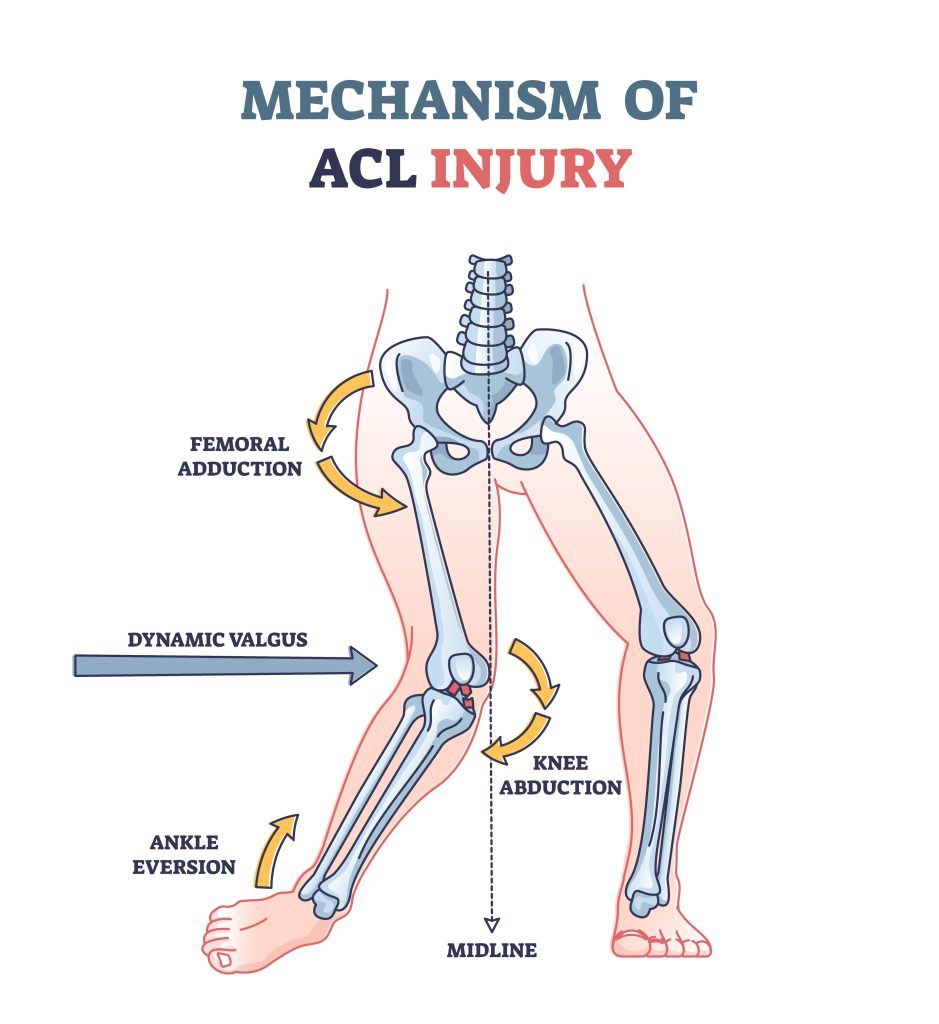
The ACL is the most commonly injured among the four ligaments that make up the knee. It is most likely to occur when the feet remain planted during a sudden stop or sudden change in direction.
This injury frequently happens to soccer, basketball, or football players. Or other sports that involve twisting your legs and knees. That’s why most ACL tears occur without contact.
You can also tear the ACL after landing awkwardly from a jump. Although it may not be painful, tearing a ligament can cause a loud popping sound.
PCL
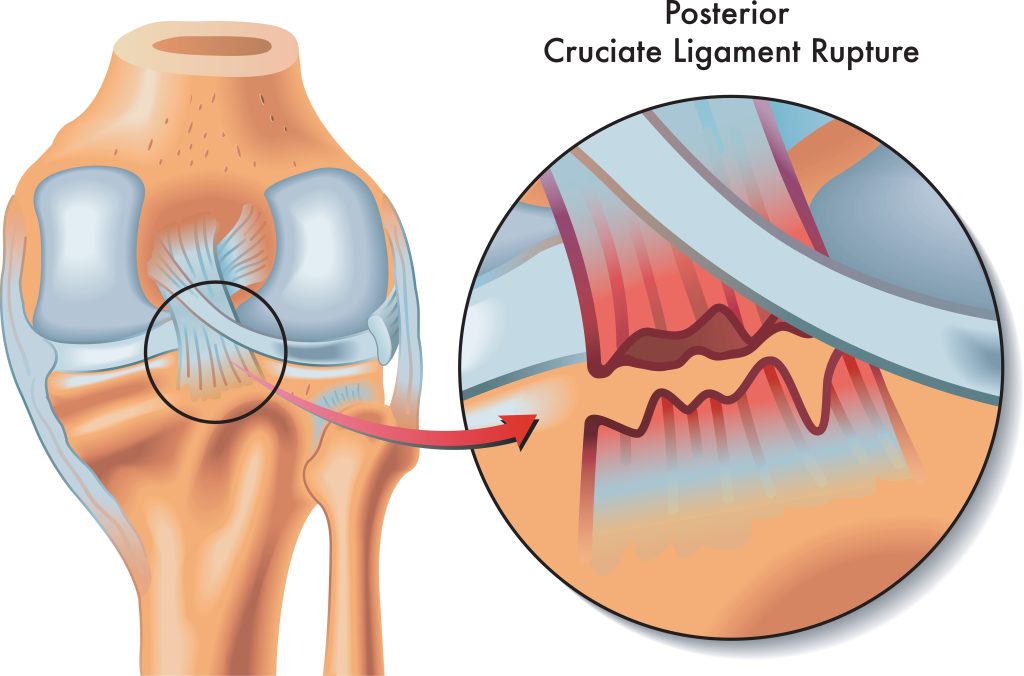
A PCL injury is somewhat less likely to occur. It usually occurs with a direct impact outside the knee joint. It’s common for front seat passengers when their knee jams into the dashboard during a car crash.
In soccer or football, this accident can happen when there’s a direct blow on the front of the tibia. A misstep on uneven ground can also cause this injury. Or when the knee hyperextends during an awkward landing. Some patients recover by modifying their activity and doing focused muscle conditioning.
Symptoms
ACL
ACL injuries lead to rotational instability. After an ACL tear, you may be able to walk, even run, in a straight line, but when you turn, you collapse.
Other causes include:
- If you shift your knee while your feet remain planted, you hear a loud popping sound
- Knee pain
- Difficulty walking
- Knee instability
- Symptoms of knee swelling
PCL
In mild injuries, people can still walk even with a PCL injury but it’s also important to know that PCL injuries can also cause knee instability and lead to difficulty in walking. ACL and PCL injury share the same symptoms, except for the popping sound associated with ACL.
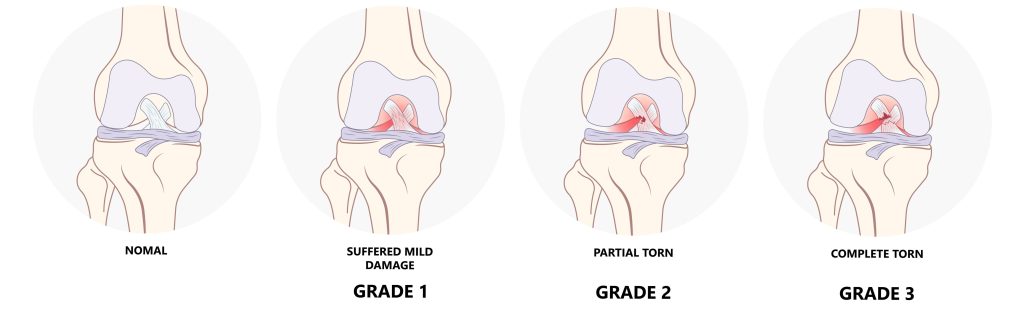
Severity of injury
The treatment for ACL and PCL injuries is similar. Still, it will differ depending on the severity, or grade, of the injury.
- 1: The ligament stretches a bit, but the knee is stable.
- 2: There is a partial tear or loosening of the ligament.
- 3: Complete rupture of the ligament.
ACL and PCL tears are painful, but the lingering instability of the knee joint is the most concerning. It is possible to overcome discomfort and instability by rehabilitating the knee muscles. However, the ligament may need reconstruction if it has completely ruptured.
What to expect at a doctor’s visit
You’ll probably be asked these questions to describe the injury:
- What symptoms are you experiencing now?
- What were you doing at the time when it occurred?
- How did it feel?
Additionally, you will receive a physical examination. Specific tests for the ACL and PCL can be used to diagnose ligament tears. X-rays and MRIs can be used to determine tissue or bone damage.
Physical Examination

Your doctor will check if there is swelling and tenderness in your knee. They may also move your knee in different positions to assess the range of motion. Understanding the nature and mechanism helps differentiate different types of injuries. A reduction in range of motion and difficulty bearing weight are typical symptoms.
Diagnostic Examination
Doctors may rule out a bone fracture with x-rays, but ligaments and tendons are not visible.
An MRI scan is the gold standard for diagnosing PCL injuries and related conditions. You can see images of soft and hard tissues using radio waves and magnetic fields. It can also reveal ACL injuries and cartilage damage.
To diagnose knee injuries, ultrasound uses sound waves to visualize internal structures.
Special Tests
ACL
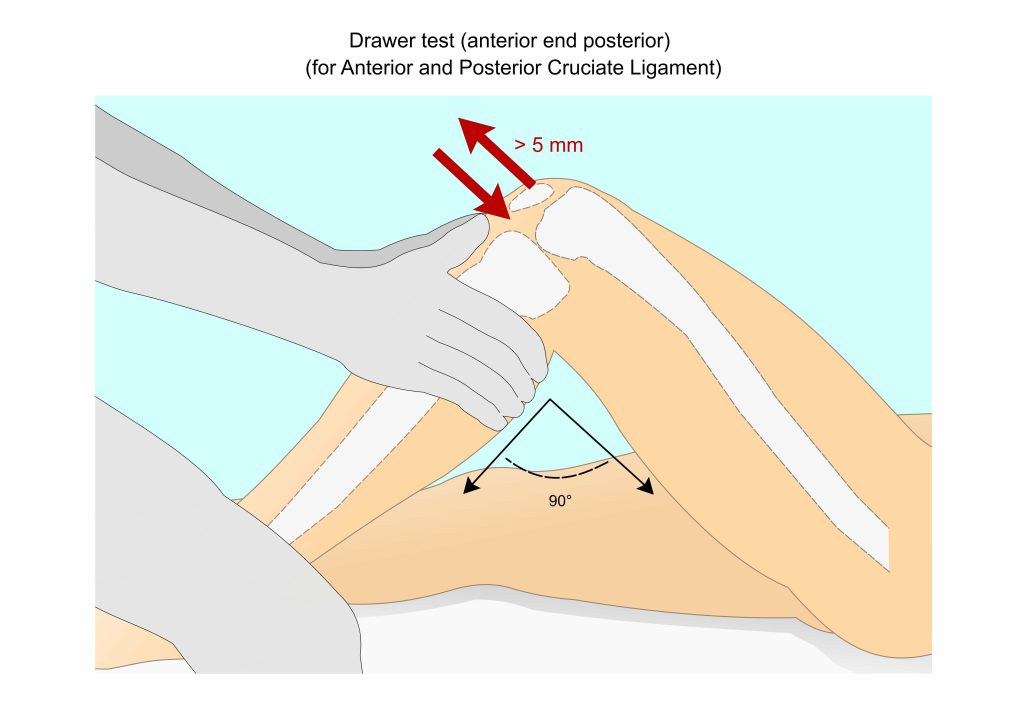
An anterior drawer test determines the integrity of a ligament. To stabilize the foot, one sits on it while bending the knee 90 degrees. Using both hands, grasp the proximal tibia firmly. Forcefully pull it anteriorly, noting any pain, laxity, or abnormal movement.
The Lachman Test assesses anterior tibia translation to the femur. Place your injured knee in 20-30 degrees of flexion while lying in a supine position. This position relaxes the iliotibial band. The examiner grips the proximal tibia with one hand. The other hand stabilizes the distal femur. Then, apply an anterior force to the proximal tibia while keeping the femur stable. A positive test means too much anterior translation on the proximal tibia. And it doesn’t have a firm endpoint. There are three endpoints: hard, soft, and absent.
The pivot shift test is an excellent test for diagnosing rotatory instability. It will determine whether a patient has symptomatic ACL tears. The examiner applies an internal rotation and valgus force to the extended knee. If the ACL is torn, the tibia will usually sublux anterolaterally. A positive test indicated that the tibia is reduced by flexion when subluxated. If you have any underlying laxity, you must always compare the results.
PCL
A posterior drawer test is the best method for assessing PCL. It has the highest sensitivity and specificity among all the tests for PCL. It is only done if there’s no swelling in the knee. PCL injury is suspected if the posterior tibia is soft or if unable to palpate this 1 cm step-off. A positive sign indicates a 10mm posterior translation.
The posterior translation of the Lachman test indicates a posterolateral ligament complex injury.
Posterior sag sign: In a positive test, the tibia sags posteriorly.
An active quadriceps test can also help diagnose a complete PCL tear.
A positive tibial external rotation test indicates an increase in external rotation at 30 degrees.
Consult your doctor about the best treatment options for your injury. They will develop a plan for getting you back to your regular activities.
Non-surgical Treatment
ACL
To treat a minor ACL tear, your doctor may suggest:
- The RICE protocol is an acronym for Rest, Ice, Compression, and Elevation. It is a combination of techniques used to treat injuries and other types of pain. These are the basic steps to reduce pain and swelling after an injury or trauma.
- During treatment, your doctor may recommend a brace to prevent the tibia bone from sagging backward.
- A crutch may help protect your knee further by preventing your leg from putting any weight on it.
- To reduce swelling and speed recovery, take anti-inflammatory drugs such as ibuprofen.
PCL
- Take a break from aggravating activities.
- If necessary, use crutches.
- During the first 48 hours, rest completely.
Rehabilitation
Rehabilitation is crucial in returning to your daily activities, regardless of whether surgery is involved. A ligament injury’s severity determines how long it will take you to recover. Combined injuries usually take a long time to heal, but most people fully recover.
When you have had surgery, you will begin physical therapy one to four weeks after your procedure. The recovery time for a job that requires a lot of physical activity can be up to 12 months.
Rehabilitation is a long process. Your commitment to therapy is crucial to get back to everything you love.
ACL Rehabilitation
Begin with early rehabilitation exercises while being mindful of controlling the swelling. Normalize your walking pattern and activate your muscles despite some pain and stiffness. Ultimately, you will work towards a full range of movement in the knee.
- Static quadriceps setting (sitting): Sit on the floor. Tense your right thigh muscle by actively tightening/squeezing it. Notice that as you do so, your leg straightens slightly. Now relax. Repeat it all over again.
- Quadriceps setting (with a towel): Sit on the floor and place a rolled-up towel under your knee. Tighten your thigh muscle by pressing your knee against the towel. Slowly return to the start position.
- Half-squat: Bend your knees to the 1/2 squat position. Ensure the middle of the knee cap lines up with the middle toes of your foot. The next step is progressing to chair squats as you become more comfortable.
- Box step exercise: Step onto a box or step, and place both feet on the step. Then, step down using the same foot as the lead leg. You can advance to a wobble balance stand with time and practice.
- One-leg balance exercise: Stand on one leg and balance yourself while holding on to a wall as you begin. Be cautious when starting this exercise to ensure balance. This exercise improves balance and strengthens your muscles, ligaments, and joints. Progress to one-leg calf raises when you get more comfortable.
PCL Rehabilitation
- In heel slides, you lie on your back and bend your knees. Make sure your foot stays in contact with the floor. You can increase your ROM by using a towel or resistance bands to pull your leg further.
- Quadriceps setting: Lie on your back and place a rolled-up towel under your knee. Tighten your thigh muscle by pressing your knee against the towel. Slowly return to the start position.
- Calf raises: On a stepper, keep your legs straight as you raise your calf up and down on your toes. Lean on the wall or hold anything for support. You can progress this exercise by doing single-leg calf raises. And then advance to single-leg calf raises without support .
- Hamstring curls: Initially, curl your hamstrings against a wall without weight. Then, use a rehabilitation band. Curl up against resistance and back down in one smooth movement. As strength and resistance increase, you may switch to a leg-press machine.
- Lunges: Using a medicine ball, perform a lunge by standing one leg in front of the other. Lean forward, and return to standing. Make sure your stomach muscles remain firm.
Surgery
You may need surgery if:
- As a result of the injury, your knee buckles during everyday activities.
- Your knee also has more than one injured ligament or fibrous cartilage.
- You are an athlete who desires to continue competing in your sport.
A graft replaces the damaged ligament, which is a segment of the tendon that connects muscle to bone. ACL tears do not always require surgery. Often, inactive people can manage with a knee brace or assisted mobility device.
Is ACL worse than PCL?
While both tears are insufferable, ACL is considered the worst and most common knee ligament to tear. ACL tears often need surgical intervention to ensure full recovery, while PCL injuries result from direct trauma, so they can be rehabilitated without surgery.
ACL is also smaller and weaker than the PCL, which means it is more likely to experience a complete injury or tear.
Conclusion
In general, there’s no set time frame for athletes to return. During rehabilitation, doctors and physical therapists will determine whether your knee is ready to resume sports activity. Before returning to an activity that could result in any injury, it is crucial to optimize strength, stability, and movement patterns.
A Note From Gulf Physio
We hope you’ve enjoyed learning about the subject matter above. This blog post is not a substitute for medical advice. The author cannot guarantee the accuracy of the information presented. If you have any questions or concerns, please consult a healthcare professional. All decisions and actions you make are your own. No one involved in making this resource is liable for its use.